diagnosis
If symptoms of anemia are observed, the patient may be sent in for testing. This typically has two parts: a complete blood count and a peripheral blood smear.
Complete blood count (CBC) A modern complete blood usually involves taking a sample of the patient's blood and running the blood through an automated counter. The counter usually records the following:
|
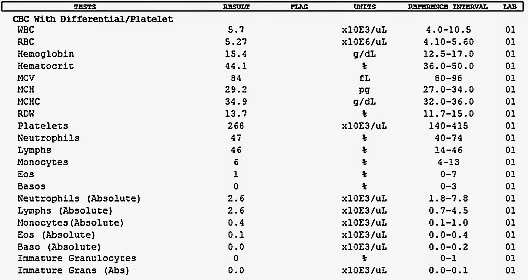
An example of a complete blood count report

An automatic counter for the CBC
|
If the total hemoglobin is significantly lower than normal (normal hemoglobin levels are 120g/L-160g/L for women and 140g/L-180g/L for men), and the hematocrit is also lower than healthy (healthy levels that are 45% for men and 40% for women) indicates anemia. The other numbers on the CBC can help determine what kind of anemia the patient has; for example, a low MCV, a high RDW, a low MCH, and a slightly higher than normal platelet count is characteristic of iron-deficiency anemia. Also, low numbers of everything (WBCs, RBCs, platelets) may indicate aplastic anemia.
Peripheral blood smear

prepared blood films/peripheral blood smears
|
A peripheral blood smear (or a blood film) involves making a microscope slide of a single drop of blood and examining the feathered edge of the smear. This doesn't provide any usable quantitative information about the patient's blood, but it allows the doctor to examine the blood cells and take a look at their shape, colour, etc. Often, anemic blood cells will have obvious differences from healthy blood cells For example, the appearance of hypersegmented neutrophils in the blood is a sure indication of megaloblastic anemia. Also, appearances of target cells indicate thalassmias.
|
Clinical History
The results from the blood tests are usually corroborated with the person's clinical history. If the patient is anemic, has a low MCV, has small, pale RBCs, and has really heavy periods, the doctor will most likely say that she has iron-deficiency anemia. In a similar fashion, if the patient is anemic, has a high MCV, and has had parts of their ileum removed, then he/she most likely has megaloblastic anemia. Everything from genetics to diet to past medical operations to drug use must be considered in a diagnosis.
Treatment
For deficiency anemias, the usual approach to treatment is either a change of diet, oral supplements, or, in cases of digestive issues, supplement injections. This method of treatment is frequently used in iron-deficiency anemia and megaloblastic anemia.
However, with more serious anemias that are genetic and/or permanent, blood transfusions are usually needed. Blood transfusions increase the number of healthy red blood cells in the blood, alleviating the effects of anemia for a certain amount of time (two months is the approximate lifespan of a RBC). Regular blood transfusions are often needed in cases of moderate to severe thalassmia. However, blood transfusions can result in even worse iron buildup in thalassmias.
For severe cases of thalassmia and aplastic anemia, a bone marrow transplant is the only lasting solution to the disease. A transplant gives the person's blood the ability to regenerate healthy blood cells, instead of just getting them from an external source (blood transfusions). However, transplants may cause rejections and autoimmune responses, where the white blood cells in the transplanted bone marrow attack the cells of the patient.
However, with more serious anemias that are genetic and/or permanent, blood transfusions are usually needed. Blood transfusions increase the number of healthy red blood cells in the blood, alleviating the effects of anemia for a certain amount of time (two months is the approximate lifespan of a RBC). Regular blood transfusions are often needed in cases of moderate to severe thalassmia. However, blood transfusions can result in even worse iron buildup in thalassmias.
For severe cases of thalassmia and aplastic anemia, a bone marrow transplant is the only lasting solution to the disease. A transplant gives the person's blood the ability to regenerate healthy blood cells, instead of just getting them from an external source (blood transfusions). However, transplants may cause rejections and autoimmune responses, where the white blood cells in the transplanted bone marrow attack the cells of the patient.
