Red blood cells are formed in the bone marrow, where they divide and differentiate from stem cells. Megaloblastic anemia is when those stem cells cannot replicate their DNA (due to a lack of folate or vitamin B12), leading to cell growth without division. This results in immature, large, and fragile red blood cells in reduced numbers.
Causes
Megaloblastic anemia is caused either by a lack of folate or vitamin B12. Folic acid directly takes part in DNA synthesis, therefore lack of it causes megaloblastic anemia. Vitamin B12, in contrast, is responsible for recycling folate for use in DNA synthesis, therefore lack of it effectively causes folic acid deficiency.
Causes of these deficiencies include:
Causes of these deficiencies include:
- insufficient dietary intake
- pernicious anemia (vitamin B12 deficiency from lack of intrinsic factor, a protein is essential in vitamin B12 absorption)
- intestine surgery, celiac disease, crohn's disease, tropical sprue (digestive tract problems that affect absorption)
- infection via tapeworms
- pregnancy, breastfeeding, or other activities that cause higher demands for folate than usual
- alcoholism (obstructs folate metabolism)
Symptoms
Megaloblastic anemia usually has a slow onset and may remain asymptomatic for a very long time. Some people may never develop symptoms or notice them. However, in addition to normal anemia symptoms, megaloblastic anemia can be marked by digestive problems (i.e. diarrhea).
Since vitamin B12 also affects the production of myelin on nerve cell axons, vitamin B-12 megaloblastic anemia (often called pernicious anemia) also results in neurological complications, such as tingling hands/feet, swollen tongue, depression, anxiety, and even memory impairment.
Since vitamin B12 also affects the production of myelin on nerve cell axons, vitamin B-12 megaloblastic anemia (often called pernicious anemia) also results in neurological complications, such as tingling hands/feet, swollen tongue, depression, anxiety, and even memory impairment.
Diagnosis and treatment
|
Diagnosis involves the usual clinical history, complete blood count, and peripheral blood smear. In addition to decreased RBC count and hemoglobin levels, the volume of the RBCs will be higher than healthy (macrocytic anemia) and the reticulocyte (healthy precursors to RBCs circulating in the blood) count is decreased. The blood smear reveals large, misshapen and fragile RBCs and excessively lobed neutrophils that are signature of megaloblastic anemia. Also, measuring vitamin B12 or folate in the blood may confirm the deficiency.
For insufficient intake or increased demand, dietary supplements of vitamin B12 or folate should suffice. However, individuals who have issues with the absorption or vitamin B12 (pernicious anemia) or folate may need continuous injections of the nutrients. Obviously, for cases caused by other diseases, treatment for that particular disease is necessary. |
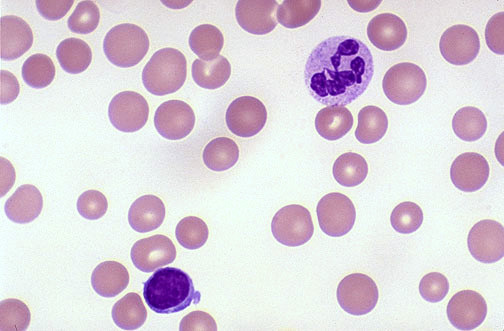
A blood smear of a patient with megaloblastic anemia: notice the neutrophil in the top right with 6 or 7 lobes instead of the usual 3 or 4
|
